New Mexico deserves credit for finally moving on several health care problems that have been obvious for years. But if state leaders want real progress, they have to admit a harder truth: this is no longer just a malpractice or hospital-management issue—it is a full system capacity problem. governor.state.nm
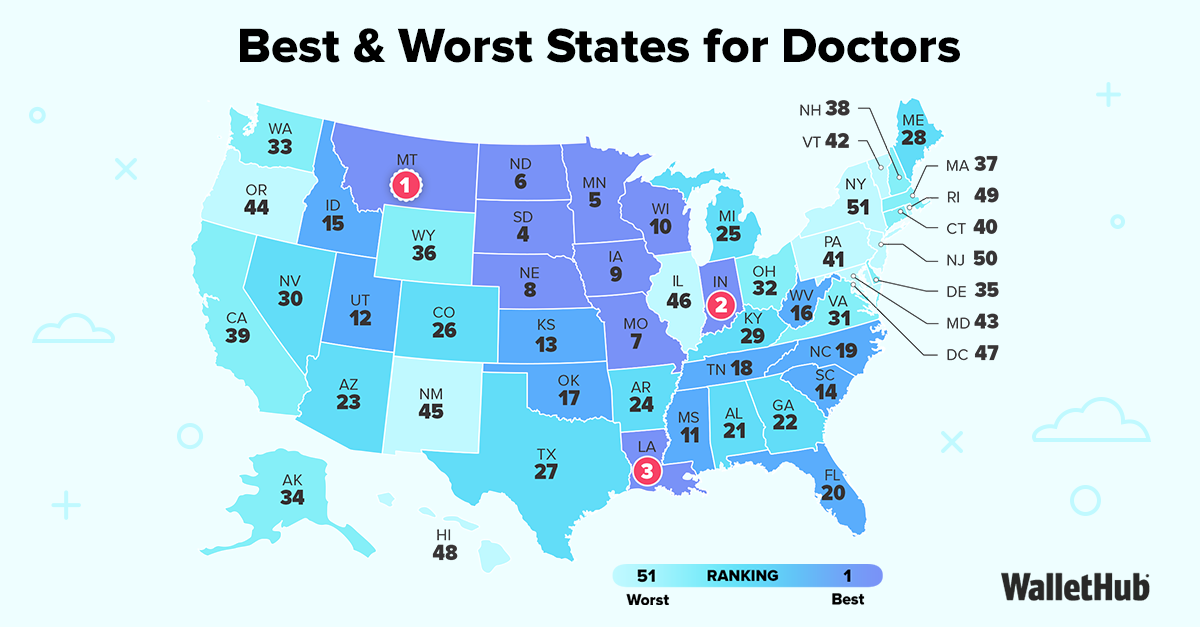
That distinction matters. WalletHub’s 2026 rankings put New Mexico 45th overall for doctors, with a noticeably worse score in “Medical Environment” than in “Opportunity & Competition,” which suggests the state’s core problem is not that physicians are unwanted, but that practicing medicine here is harder than it should be. New Mexico also continues to face a deep workforce shortage, with all but one of its 33 counties designated as health professional shortage areas and analysts warning the broader health-care worker gap could worsen by 2030. mentalfloss
To be fair, lawmakers did not ignore the problem this year. The governor signed a package that included malpractice reform, more funding support through the Health Care Affordability Fund, and limits on certain outpatient facility fees, while the state also moved forward with the Interstate Medical Licensure Compact to make it easier for out-of-state physicians to practice here. Those are real reforms, and they deserve recognition because recruitment, affordability, and physician supply all matter. kunm
But New Mexico’s medical system is under pressure from more than licensing and liability. The Hospital Patient Safety Act requires hospitals to submit recurring staffing plans for nursing, professional, technical, and service workers as a condition of licensing, which tells you lawmakers themselves recognized staffing and patient safety had become structural issues, not isolated complaints. At the same time, UNM Hospital has had to build a dedicated Workplace Violence Program, install metal detectors in the emergency department, expand security operations, and rely on 115 proprietary security officers and more than 2,000 cameras to protect staff and patients. nmlegis
That is not normal system maintenance. That is what it looks like when a hospital is being asked to function as a trauma center, psychiatric intake point, security zone, and social-services fallback all at once. New Mexico’s own Department of Health reported that from 2019 to 2023, 30,882 hospital patients were experiencing homelessness, which shows how directly housing instability and social disorder flow into clinical settings. The state’s behavioral-health assessment also says New Mexico needs more transitional housing, faster referrals, and more medical respite capacity for homeless and medically vulnerable patients, which is another way of saying too many people are being discharged into circumstances that make recovery harder and readmission more likely. hscnews.unm
This is where the conversation usually goes off the rails. It is too simplistic to say immigrants, homeless patients, or public-benefit recipients are “the problem.” The better argument is that New Mexico has built a public system in which hospitals and clinics are routinely expected to absorb the consequences of failures in housing, behavioral health, addiction treatment, and social stability. The state has also expanded protective immigrant policies through measures like the 2026 Immigrant Safety Act and reinforced institutional support through the Office of New Americans, while continuing to use state resources to cushion coverage and food-support disruptions. Those choices may reflect compassion, but they also add to a wider public-service load in a state whose provider base is already thin. san
Patients feel that strain even when they are insured. New Mexico approved an average 35.7 percent increase for 2026 ACA individual-market plans, with regulators citing higher medical costs, higher prescription-drug costs, and heavy service utilization. The state has used subsidies to cushion many marketplace enrollees from the full premium hit, but subsidies do not erase the underlying cost—they just move more of it onto taxpayers and state funding streams. Meanwhile, patients still face the access side of the crisis: long waits, delayed referrals, specialist shortages, and the frustration of having coverage without timely care. osi.state.nm
That means insured New Mexicans may be paying into a system that is more expensive and less convenient at the same time. It does not necessarily mean the doctors are worse. It means the system around them is overstretched. news.unm
So what should leaders do next, beyond taking a victory lap for the bills they already passed? First, build a statewide medical-respite network for medically fragile homeless patients so hospitals are not forced to serve as improvised recovery housing. Second, pair the licensure compact with serious residency expansion and rural specialist incentives, because easier licensing helps recruitment but does not solve the in-state pipeline problem by itself. Third, make workplace violence prevention a statewide standard with reporting, security upgrades, panic-alert systems, and post-incident support rather than leaving each hospital to improvise. Finally, create a transparent public dashboard tracking vacancies, ER wait times, psychiatric boarding, discharge delays, and staff assaults so New Mexicans can see what overload actually looks like. kunm
New Mexico’s leaders have started to address the health-care crisis, and they should get credit for that. But unless they reduce the outside burdens flooding hospitals—shortages, violence, homelessness, behavioral-health instability, and discharge bottlenecks—they are still asking a thin medical workforce to carry a social services-heavy state on its back. nmhealth
These problems aren't just a blip. New Mexico's rank is sh*tty every year. How does a problem like this endure? -Leadership.

Change to GOP or Indie here in 3m